
Can Reminders Boost Vaccination Rates?

Context
In recent years, Guatemala has implemented supply-side interventions to boost vaccination rates: vaccines are provided free, and consistent efforts are being made to ensure that they are always available. In the mid-1990s, the government established the Coverage Extension Program (PEC), a program providing free basic healthcare services to children under the age of five and women of reproductive age, with a focus on preventive care. The Ministry of Health then hired local nongovernmental organizations (NGOs) to operate a network of rural basic clinics in which health workers are expected to track individual families and inform them when they should attend the monthly mobile medical team’s visit. However, there are no clear guidelines and communication depends on the health workers’ initiative.
As a result of these combined efforts, vaccination rates have increased dramatically. However, while coverage rates for vaccines due in the first months of life are high, they decrease markedly for vaccines due after children turn one year of age. These patterns suggest that families recognize the value of vaccination and may be willing to incur the (time) costs involved in having their children vaccinated, but often fail to follow through with their plans to complete the vaccination cycle.
The Project
Data suggest that families in rural Guatemala recognize the value of vaccination by getting their children vaccinated at early ages, but fail to follow through with their plans as their children get older. In this experimental intervention, community health workers were given monthly lists of children due for vaccination at the clinic, enabling them to send timely reminders to families.
Behavioral Analysis
Behavioral Barriers
Present bias: It is the tendency to choose a smaller gain in the present over a large gain in the future. It is related to the preference for immediate gratification. It is also known as hyperbolic discounting. People with such a bias might value present gratification more than greater benefits in the future—for example, they might avoid or delay the getting their children vaccinated even when in the future this could result in complications resulting from a disease.
Hassle factors: Seemingly small inconveniences, such as having to read a lot of information or take an extra small step to complete an action, can hinder or disrupt decision-making processes. In this context, even if parents have become fully aware that they should get their children vaccinated, it takes only a few simple “obstacles” for them to desist from their intention.
Optimism bias: It leads us to underestimate the probability that negative events will happen to us and to overestimate the probability of positive events (i.e., parents may overlook the probability that their children can get a specific disease).
Availability heuristics: Individuals tend to estimate the probability of a future event based on how readily representative examples of such an event come to mind. Parent’s tendency to underestimate the probability of their children getting sick from a preventable disease may be based on examples that come to their minds.
Behavioral Tools
Reminders: They can take many forms, such as an email, a text message, a letter, or an in-person visit reminding individuals of some aspect of their decision-making process. Reminders are designed to mitigate procrastination, oversight, and cognitive overload. Providing reminders can encourage parents to keep in mind the importance of children’s vaccination.
Intervention Design
The intervention consisted of randomly assigning 130 basic clinics operated by NGOs under PEC to a treatment or a control group. In treatment communities, health workers received lists of children who were due to receive a vaccination at the clinic in the following month, enabling them to send timely reminders to families.
The lists were distributed to community health workers at monthly meetings at the NGO offices, along with information on the medical team’s upcoming visit to their clinic. While health workers in all PEC communities are expected to provide some kind of reminder, health workers in treatment communities received concise, up-to-date information regarding which families to remind, whereas health workers in control communities had to rely on their own records, which they may or may not have created and maintained. The specific type of reminder depended on the initiative of the workers. After six months of implementation, the rate of children who had received all vaccines recommended for their age was compared across groups.
Challenges
- To implement the intervention, a software developer wrote a program that produced the lists of patients due for preventive health services. Additional staff were hired to produce the lists every month in each of the four study areas for the clinics that were randomly assigned to the treatment group. These four staff members were aware of the study’s experimental design and understood that they should not distribute the lists to clinics assigned to the control group. At the community health workers’ monthly meetings at the NGO offices, facilitators distributed the lists with information on individuals in their communities who needed health services that month and the following month to the treatment group. Community health workers in the control group were aware of the study and may have observed the lists being distributed to health workers in the treatment group. If this fact made health workers in the control group increase their efforts to track patients in their coverage areas, this would lead to underestimating the treatment effects of this study.
Results
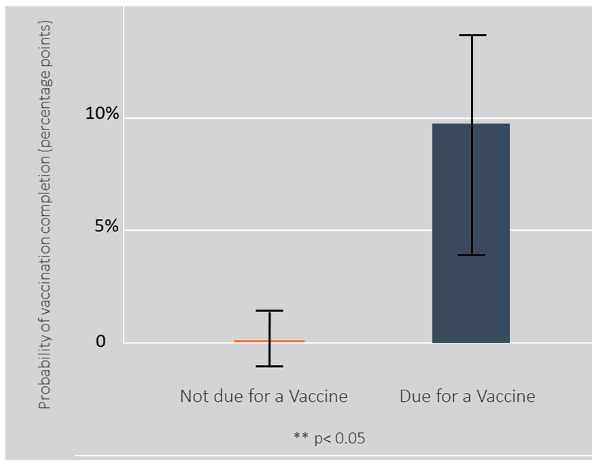
The intervention increased the probability of vaccination completion by 2.2 percentage points among all children in treatment communities (ITT). For children in treatment communities who were due to receive a vaccine and whose parents were thus expected to be reminded about that due date, the probability of vaccination completion increased by 4.6 percentage points (figure 1). The LATE estimate shows a stronger effect, increasing the probability of complete vaccination by 4.5 percentage points for all children in treatment communities and 9.1 percentage points for children due for a vaccine (figure 2). Estimated effects for children of parents not expected to be reminded are essentially zero, suggesting that the intervention did not generate spillovers for these children within treatment communities.
The overall effects of providing reminders are remarkable in light of its low cost. The estimated total cost of scaling up this intervention in Guatemala is only $0.17 per child for the six-month intervention. Hence, the cost per additional child with complete vaccination due to this intervention is expected to be around $7.50. Reminders were found to be a cheaper tool than others (such as conditional transfers) to increase immunization. The low cost-benefit ratio makes this a scalable option for other goals, such as malaria.
Figure 1. ITT on Achieving Complete Vaccination
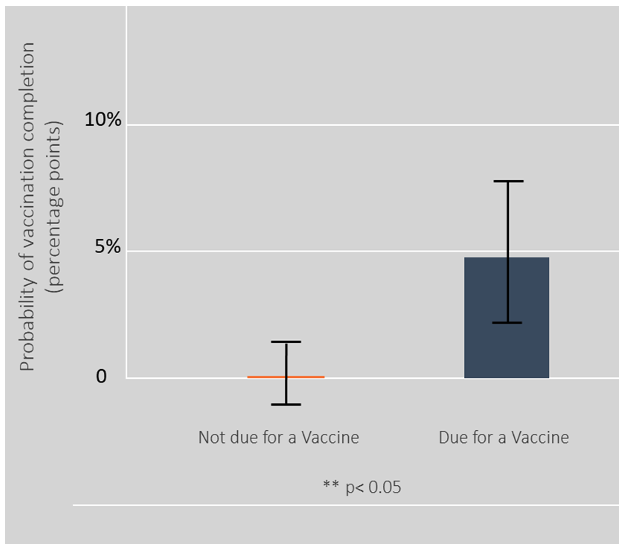
Figure 2. ITT on Achieving Complete Vaccination
Policy Implications
- The project offers evidence of the promising role of reminders on demand for preventive health services. There is an opportunity to expand the role of reminders to achieve further gains in vaccination rates at a moderate cost.
- Moreover, reminders could potentially be used not only to increase vaccination levels, but also to spur demand for other preventive healthcare measures. For example, it is well documented that insecticide-treated bed nets can substantially reduce child mortality in developing countries where malaria is prevalent.