
Delivering Parenting Interventions through Health Services in the Caribbean

Context
In low- and middle-income countries, many children under the age of five do not achieve their full potential development due to risks associated with poverty, malnutrition, and inadequate stimulation. It has been recommended to integrate early childhood development interventions into health and nutrition services. However, information on which interventions are most effective, and feasible to be delivered through health services, is limited.
The Project
The project is a field experiment in a cluster randomized by public health center in three Caribbean countries. We developed an early childhood stimulation program that could be delivered to groups at routine primary health-care visits for immunizations, and evaluated the benefits in terms of enhancing parents’ knowledge, the amount of stimulation provided to children, and children’s developmental levels.
Behavioral Analysis
Behavioral Barriers
Status quo bias: It is the tendency to maintain the current state of affairs, even when change is clearly better. This current status, or status quo, is used as a reference point, and any change with regard to this reference is seen as a loss. In this context, not taking actions to support their children’s development).
Present bias: It is the tendency to choose a smaller gain in the present over a large gain in the future. It is related to the preference for immediate gratification. It is also known as hyperbolic discounting. People with such a bias might value present gratification more than greater benefits in the future—for example, they might avoid paying taxes even when there is a possibility of winning a lottery. In this context, parents may be biased towards not taking the time to invest in their children’s development because the rewards are in the long term.
Behavioral Tools
Framing: The way in which information is presented influences people’s conclusions. For example, options may be presented in a way that highlights their positive or negative aspects, leading each to be perceived as relatively more or less attractive.
Intervention Design
In the Caribbean, maternal and child health clinics are based in primary-care health centers and are typically held once a week. A parent training package was delivered to mothers of babies aged 3 to 18 months in routine clinics without requiring additional staff and was designed to occupy the time the mothers spent waiting to see a nurse. The package was comprised of videos, followed by a discussion with a demonstration, and time for practicing several activities, as well as the provision of message cards and a few play materials to take home.
The videos delivered a series of child development messages. Nine modules were produced, each approximately three minutes in length, covering the topics: (1) love, (2) comforting a baby, (3) talking to babies and children, (4) praise, (5) using bath time to play and learn, (6) looking at books, (7) simple toys mothers can make, (8) drawing and games, and (9) puzzles.
Figure 1. Illustrations from the Treatment
A cluster randomized trial was conducted in 29 Caribbean health centers, stratified by country (Jamaica, Antigua, and St. Lucia). Health centers were assigned to either a control group (n=15) or to an intervention group (n=14). Primary outcomes (children’s cognition, language, and hand-eye coordination) and secondary outcomes (caregiver knowledge, practices, postpartum depression, and child growth) were measured after the 18-month postpartum visit.
Challenges
Training and engagement of medical staff is key: Community health workers (CHWs) and nurses were trained to discuss the videos’ messages with mothers and demonstrate the activities they had seen. A manual was provided to CHWs that included program objectives, guidelines for engaging mothers in the discussion and demonstration sessions, and recommended content for each session. CHWs were trained in workshops, followed by coaching in clinics by a supervisor from the research team, which also monitored the quality of implementation.
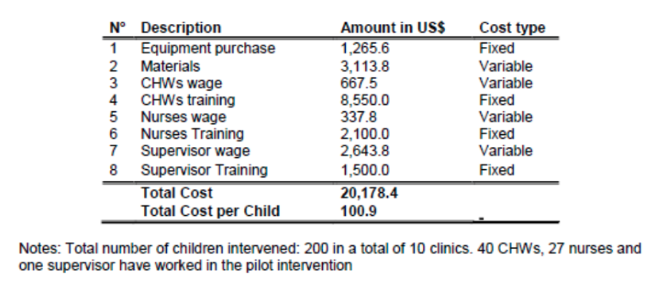
The main implementation challenges related to staff workload and managing groups during the training of medical staff. Table 1 offers a breakdown of the intervention costs.
Table 1. Intervention Costs
Results
Multilevel analyses show that the health center intervention had significant benefits for children’s cognitive development and mothers’ parenting knowledge (figure 2).
- The average scores for children at intervention health centers after their 18-month visit was higher than children at control health centers, a difference equal to 0.3 standard deviations.
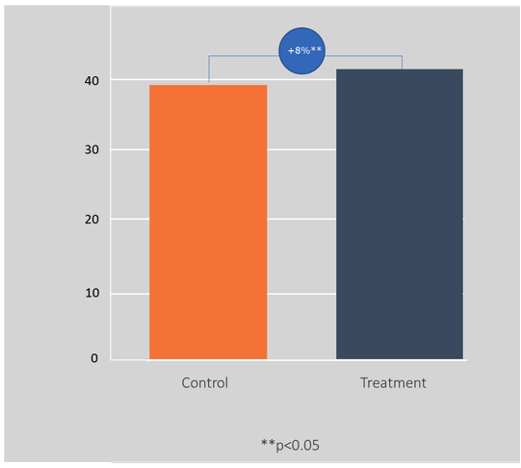
- Mothers in the intervention group improved significantly more in their scores for knowledge and attitudes concerning child development than mothers in the control group, an effect of 0.4 standard deviations.
- Qualitative interviews confirmed that both mothers and health staff perceived intervention benefits for the mothers themselves and their children.
- Furthermore, this intervention is cost-effective. The most conservative analyses found a benefit-cost ratio of 5.3.
Figure 2. Cognitive Development
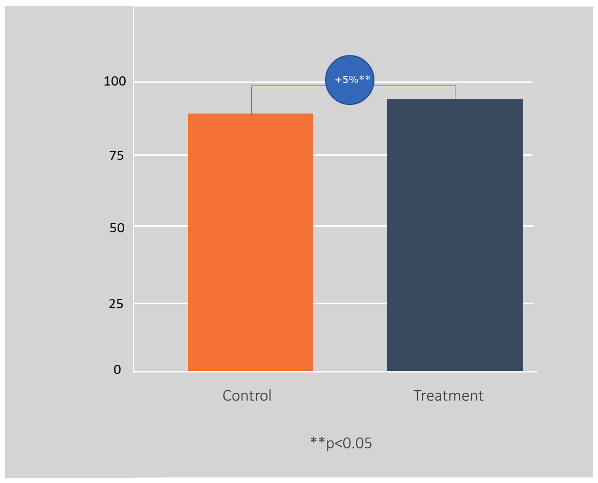
Figure 3. Parenting Scores
Policy Implications
- The arguments present in the study are based on economic calculations, which are important because this is precisely the type of calculation that officials in the Ministry of Finance and Planning Commission make.
- Using a variety of media to communicate key messages, and scheduling their delivery for a time when recipients are already present (in this case, waiting for a nurse in a waiting room), are both key elements of the intervention’s success, with implications for other policy interventions.